The Adult ADHD Self-Report Scale version 1.1 (ASRS v1.1) is an 18-item self-report screening instrument for adult ADHD, developed through a World Health Organization initiative and validated by Kessler et al. in 2005. It is the primary screening questionnaire used in adult ADHD assessments in Australia, and the instrument Velluto digitises for pre-consultation intake.
Quick links
- At a glance
- What is the ASRS v1.1 and what does it measure?
- How is the ASRS v1.1 structured?
- What is the clinical threshold and what does it mean?
- What does proper administration require?
- Question order, fatigue and context
- What does digital delivery change?
- What does Velluto do with the ASRS?
- Frequently asked questions
At a glance
| Feature | Detail |
|---|---|
| Developer | World Health Organization / Kessler et al. |
| Year | 2005 |
| Items | 18 (plus a 6-item screener subset) |
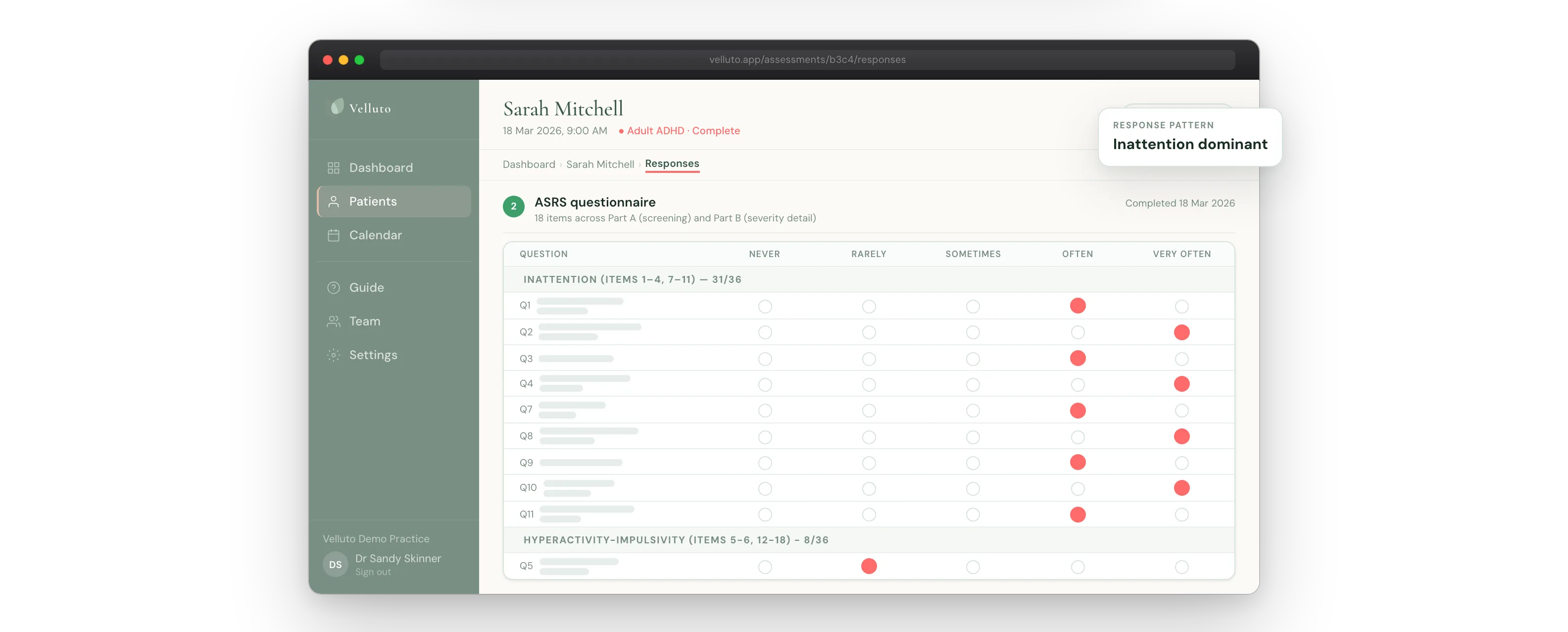
| Subscales | Inattention (9 items) and hyperactivity-impulsivity (9 items) |
| Response format | 5-point frequency scale (Never / Rarely / Sometimes / Often / Very often) |
| Maximum raw score | 72 |
| Clinical threshold | 5 or more of 9 symptom items scoring at the clinical level |
| Administration time | Under 5 minutes on average |
| Who completes it | The patient (self-report) |
| Diagnostic status | Screening instrument only. Not a diagnostic tool. |
What is the ASRS v1.1 and what does it measure?
The ASRS v1.1 measures self-reported frequency of ADHD-related behaviours in adults. Each of the 18 items maps to one of the DSM-5 symptom criteria for ADHD: nine items for inattention, nine for hyperactivity-impulsivity. The instrument asks how often certain behaviours occur using a five-point frequency scale from Never to Very Often.
The scale does not measure severity in the clinical sense. It measures frequency of self-reported behaviour. A high total score does not mean the patient has ADHD. A low score does not rule it out. The ASRS is a data collection instrument. The GP makes the clinical assessment.
The ASRS was developed under a WHO initiative as part of the World Mental Health Survey project. The validation paper (Kessler RC et al., 2005, Psychological Medicine) established its psychometric properties using a sample of 154 respondents from the US National Comorbidity Survey Replication. Kessler and colleagues identified a 6-item screener subset within the 18 items that performed well against blind clinical diagnoses: sensitivity 68.7%, specificity 99.5% for that subset. The full 18-item scale has been used clinically since and is the form that appears in Australian practice.
How is the ASRS v1.1 structured (items, subscales, and scoring)?
The 18 items divide evenly into two subscales:
- Inattention subscale (items 1-9): covers difficulty sustaining attention, making careless errors, failing to finish tasks, difficulty organising, avoiding tasks requiring sustained mental effort, losing things, being distracted, forgetfulness in daily activities, and difficulty listening when spoken to directly.
- Hyperactivity-impulsivity subscale (items 10-18): covers fidgeting, leaving seat inappropriately, running or climbing when it is not appropriate (adapted for adults: feelings of restlessness), difficulty playing quietly, being “on the go”, talking excessively, blurting out answers, difficulty waiting a turn, and interrupting others.
Each item is scored on a 0-to-4 scale corresponding to the five frequency options. Total raw scores run from 0 to 72. Subscale scores run from 0 to 36 each.
The threshold is based on symptom count, not total score. Rather than using the summed raw score as the primary clinical signal, the ASRS threshold counts how many individual items score at or above a clinically meaningful frequency. The standard cutoff used in Australian clinical practice requires five or more out of nine relevant symptom items to score at the clinical level to meet the inattention or hyperactivity-impulsivity criterion, consistent with the DSM-5 diagnostic threshold.
Scoring is arithmetic. There is no algorithm, no weighting by item, and no clinical judgement involved in calculating the score. The GP receives the score; the GP interprets it.
What is the clinical threshold and what does it mean?
A score at or above the threshold on either subscale indicates clinically elevated self-reported symptom frequency for that domain. It does not indicate a diagnosis. It means the patient has reported, at a frequency consistent with the diagnostic criteria, that these symptoms occur in their daily life.
The threshold is a starting point for clinical assessment, not an endpoint. ADHD assessment requires corroboration across multiple data sources: collateral observer reports, childhood onset evidence, documented functional impairment, and clinical interview. The ASRS score is one input.
What the threshold does not tell you:
- Whether another condition (anxiety, sleep disorder, thyroid dysfunction, depression, trauma history) accounts for the symptom frequency
- Whether the patient has insight into their own behaviour and reported accurately
- Whether the frequency reported reflects current state or historical baseline
- Whether the behaviour has been present since childhood, which DSM-5 requires
The AADPA Clinical Practice Guideline for ADHD (2022) positions the ASRS as a screening instrument that supports, rather than replaces, full clinical assessment. A positive screen should be followed by structured clinical assessment. A negative screen does not rule out ADHD when clinical presentation is compelling.
What does “proper administration” require in general practice?
Administration conditions matter. A self-report instrument is only as reliable as the conditions under which it was completed. GPs who have not previously used the ASRS in practice sometimes underestimate how much the administration context affects the data.
Setting
The patient should complete the ASRS without assistance from anyone else and without the GP present during completion. Presence of a clinician during self-report creates social desirability effects: patients modulate their answers based on perceived expectations. The patient should complete the questionnaire privately, with adequate time, and without interruption.
Explanation before completion
Before the patient begins, they should understand what the questionnaire is measuring and that there are no right or wrong answers. “Answer based on how often you have experienced these things, not how you want to be seen.” Do not give examples of what each item looks like in practice. Examples shape answers toward or away from clinical presentations.
Literacy and language
The ASRS is validated in English. Australian practices serving non-English-speaking patients should consider validated translations where available, or arrange for appropriate language support. Patients with low literacy should be offered support, but support must not bias the answers toward clinical presentations.
Time
Rushing a patient through the questionnaire reduces data quality. Under Velluto’s completion speed signal (a response validity indicator), average completion time under 3 seconds per question suggests the patient did not read the items. This signal is available to the GP as part of the response validity summary; it is not shared with the patient.
Who completes it
The patient completes the ASRS. The GP does not complete it on the patient’s behalf based on clinical observation. That would shift the instrument from a self-report to a clinician-administered rating scale, which it is not.
How should question order, fatigue, and context affect how GPs administer the ASRS?
Paper administration presents all 18 items in a fixed sequence. The patient reads down the page. By items 14 through 18, some patients are fatigued and start pattern-responding. They choose the same answer for every remaining item regardless of its content. This is a known limitation of fixed-format self-report scales.
Fatigue effects
Clinical literature on self-report instruments consistently identifies primacy and recency effects: items at the start and end of a scale receive more attention than items in the middle. Items 5 through 13 are the zone of highest fatigue risk in the ASRS.
The clinical impact: if a patient pattern-responds through the middle third of the ASRS, subscale scores for that range become unreliable. The GP who receives a paper form has no way to detect this.
Question order bias
When items of similar content appear in sequence, patients sometimes anchor on their answer to the first item and answer subsequent items relative to it rather than considering each item independently. On paper, the fixed order means inattention items cluster together and hyperactivity items cluster together, which increases this anchoring risk for each subscale.
Context contamination
Patients who complete the ASRS in a waiting room alongside other patients, in a GP’s office with staff movement nearby, or on a mobile phone while managing children, are answering in conditions the instrument was not validated in. The validation studies used controlled assessment environments.
Addressing these conditions does not require the GP to redesign the instrument. It requires awareness of when the data may be less reliable, and the clinical judgement to probe further when the context was clearly poor.
What does digital delivery change about ASRS administration?
Digital administration changes several administration conditions in ways that affect data quality, sometimes for better and sometimes for worse.
What improves
When the patient completes the ASRS on their own device at their own pace, outside a clinical setting, several conditions improve. There is no waiting room noise or time pressure. The patient chooses when they are ready. There is no GP or staff presence during completion. Answers are recorded precisely, not handwritten and later interpreted.
One-question-at-a-time presentation (used in Velluto’s implementation) prevents the patient seeing the complete list of items before answering. This reduces anchoring and reduces the ability to pre-plan a response pattern based on what a “typical ADHD response” looks like.
Randomised question order presents items in a different sequence for each patient. This removes the clustering effect where all inattention items appear together and all hyperactivity items appear together. It also means no two patients see the same sequence, which reduces the impact of online answer guides that tell patients which answers correspond to a positive screen.
What introduces new considerations
Digital administration happens unsupervised and at a physical distance from the GP. The patient may complete the questionnaire with others present, or may be interrupted mid-completion. There is no clinical environment to structure the experience.
Completion speed becomes measurable in digital administration in a way paper cannot capture. A patient who completes all 18 items in under 45 seconds (under 3 seconds per item) has almost certainly not read the questions. On paper, this is invisible. In digital administration, it is a data point.
Response consistency checking
Paper administration gives no way to check internal consistency. Digital administration allows validation questions to cross-check whether a patient responded consistently. These are items paired with core ASRS items for that purpose. Velluto includes six validation question pairs in its implementation. The consistency of paired responses is one of five data quality signals the GP sees in the response validity summary.
What does Velluto do with the ASRS?
Velluto presents the ASRS v1.1 one question at a time, in randomised order, on the patient’s own device as part of pre-appointment intake. The patient completes it before they arrive for the consultation.
The implementation includes:
- 18 ASRS core items, one at a time, in randomised sequence
- 6 validation question pairs (not adjacent to their corresponding core items)
- 4 to 6 context questions in randomised placement
- Completion speed tracking (time per question, available to GP only)
- Deterministic scoring: pure arithmetic, no AI involved
The GP sees a scored result before the consultation: subscale scores, total score, symptom count, and a response validity summary covering the five data quality signals. The clinical summary does not tell the GP what the score means. It presents the data. The GP interprets it.
The scored ASRS result appears alongside the observer report, childhood onset evidence, and other clinical history in the pre-consultation summary pack. The GP arrives at the consultation with data already structured, not with a blank form to work through.
Velluto does not diagnose. The ASRS does not diagnose. The GP diagnoses.
Closing
The ASRS v1.1 is a well-validated, freely available screening instrument. Administering it properly in general practice means more than handing a patient a form. Administration conditions affect the quality of the data the GP receives. Setting, explanation, time, question format, and completion context all matter.
Digital delivery changes some of those conditions and makes others measurable. It does not resolve all of them. What changes is that the GP has more information about the quality of the data before the consultation begins.
The ASRS gives the GP a structured starting point. What happens next is clinical judgement.
Related in this series
Companion posts on how Velluto prepares the evidence before an ADHD consultation.
Observer reports in GP ADHD assessment: what they are and why they change the consultation
How observer reports change the quality of evidence before the consultation.
Childhood school reports in adult ADHD assessment
Using school reports and developmental records as childhood onset evidence in adult ADHD assessment.

Response validity in ADHD screening: the five-signal model
The five deterministic signals Velluto checks to flag data quality issues.
What a GP receives before an ADHD consultation with Velluto
What a GP receives before an ADHD consultation, scored and cross-referenced.
Frequently asked questions
What is the ASRS v1.1?
The Adult ADHD Self-Report Scale version 1.1 (ASRS v1.1) is an 18-item self-report screening instrument for adult ADHD, developed through a World Health Organization initiative and validated by Kessler and colleagues in 2005. It asks patients how often they experience ADHD-related symptoms using a five-point frequency scale. It is a screening tool, not a diagnostic instrument. The GP makes the clinical assessment using the ASRS result alongside other evidence.
How is the ASRS v1.1 scored?
The ASRS v1.1 is scored arithmetically. Each of the 18 items is rated from 0 (Never) to 4 (Very Often), giving a maximum raw score of 72. The nine inattention items and nine hyperactivity-impulsivity items form two subscales scored separately. The standard clinical threshold counts how many individual items score at or above the clinically meaningful level; five or more items in a domain reaching that level meets the DSM-5 criterion count for that symptom category.
What does a positive ASRS score mean clinically?
A positive screen on the ASRS means the patient has self-reported symptoms at a frequency consistent with the diagnostic criteria for ADHD. It does not confirm a diagnosis. ADHD assessment requires corroboration from other sources: collateral observer data, childhood onset evidence, functional impairment documentation, differential diagnosis consideration, and clinical interview. The ASRS is a starting point, not a conclusion.
What does the AADPA guideline say about the ASRS v1.1?
The AADPA Clinical Practice Guideline for ADHD (2022) positions validated self-report instruments, including the ASRS, as a component of thorough adult ADHD assessment alongside collateral information, childhood onset evidence, and structured clinical interview. The guideline notes that self-report alone is insufficient; a positive screen should be followed by full clinical assessment.
What does proper ASRS administration require?
Proper administration requires the patient to complete the ASRS independently, without assistance, without the GP present, with adequate time and without interruption. The patient should understand they are reporting frequency of their own experience, not trying to achieve a particular score. Administration conditions all affect data quality: setting, time pressure, and literacy support. Paper forms cannot capture how the questionnaire was completed; digital administration adds measurable indicators including completion speed.
Does digital administration of the ASRS produce different results than paper?
Digital administration changes several conditions: one-question-at-a-time presentation reduces anchoring and pattern-response; randomised question order removes subscale clustering; completion speed becomes measurable. Patient-facing conditions also change: completion happens at the patient’s own pace and on their own device, which removes waiting room time pressure but means the clinical setting does not structure the experience. Neither paper nor digital is categorically superior. Digital administration provides data quality indicators that paper cannot.
How does Velluto handle the ASRS?
Velluto presents the ASRS v1.1 one item at a time in randomised order as part of pre-appointment patient intake. Scoring is deterministic arithmetic with no AI involvement. The GP receives subscale scores, total score, symptom count, and a five-signal response validity summary covering self-report consistency, severity distribution, completion speed, self-report versus observer agreement, and childhood onset consistency. All results appear in a pre-consultation summary pack before the appointment begins. Velluto does not interpret the scores or make clinical recommendations. The GP uses the data.
References
- Kessler RC, Adler L, Ames M, Demler O, Faraone S, Hiripi E, Howes MJ, Jin R, Secnik K, Spencer T, Ustun TB, Walters EE. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychological Medicine. 2005;35(2):245-256. PMID: 15841682.
- Hines JL, King TS, Curry WJ. The adult ADHD self-report scale for screening for adult attention deficit-hyperactivity disorder (ADHD). Journal of the American Board of Family Medicine. 2012;25(6):847-853. PMID: 23136325.
- Australian Evidence-Based Clinical Practice Guideline for Attention Deficit Hyperactivity Disorder (ADHD). Australian ADHD Professionals Association (AADPA), 2022.
Clinical information disclaimer
This article contains general clinical information for healthcare professionals. It is not a substitute for individual clinical judgement, professional guidelines, or specific patient assessment. Always apply your own clinical reasoning when making treatment decisions.
Velluto is a clinical intake platform. It does not diagnose, recommend treatment, or make clinical decisions. All clinical decisions remain with the treating GP.