Response validity in ADHD assessment refers to whether the data a patient has reported is a reliable reflection of their actual symptom experience. A self-report questionnaire produces numbers. Response validity asks whether those numbers are worth acting on.
The question is not whether the patient is lying. It is whether the conditions under which the data was collected mean the data represents them accurately. Conditions that affect data quality include rushing through questions, answering at maximum severity out of fear of not being believed, and completing the form while distracted.
Quick links
- At a glance: the five signals
- What is response validity in ADHD screening?
- Why does response validity matter clinically?
- Signal 1: Self-report consistency
- Signal 2: Severity distribution
- Signal 3: Completion speed
- Signal 4: Self-report vs observer agreement
- Signal 5: Childhood onset consistency
- How should a GP interpret validity signals?
- Is a validity rating the same as malingering or symptom fabrication?
- What does Velluto actually do with the five signals?
- Frequently asked questions
At a glance: the five signals
| Signal | What it checks | Trigger | Applies to |
|---|---|---|---|
| V1: Self-report consistency | Validation question pairs against their ASRS counterparts | 2 of 6 pairs differ by 2+ points = REVIEW; 3+ pairs = CONCERN | Adult ASRS only |
| V2: Severity distribution | Percentage of items rated at maximum severity | More than 80 percent at max = REVIEW; more than 95 percent = CONCERN | All instruments |
| V3: Completion speed | Average seconds spent per item | Under 4 seconds per item = CONCERN | All instruments |
| V4: Self-report vs observer agreement | Absolute difference between patient and observer totals | Difference greater than 20 points = REVIEW; greater than 35 points = CONCERN | All instruments with an observer |
| V5: Childhood onset consistency | Stated age of onset against childhood self-report | Onset after age 25 or recent onset = REVIEW | Adult assessments only |
All five signals are checked automatically. Each produces a rating of OK, REVIEW, CONCERN, or NOT APPLICABLE. Results appear in the clinical summary pack. Patients never see them.
What is response validity in ADHD screening?
Response validity is a measure of whether self-reported data is credible and internally consistent. In the ADHD assessment literature, it sits alongside performance validity testing as part of what Suhr and Berry (2017) describe as “the assessment of symptom and performance validity” (Psychological Assessment). This framing reflects a recognition that self-report alone, without any quality check, is insufficient for a thorough clinical picture.
In practice, response validity checking asks questions about the data itself before the GP interprets it. Were answers given consistently? Does the severity pattern match what the clinical literature would expect from a genuine ADHD presentation? Did the patient spend long enough on each question to have read it? None of these questions produce a diagnosis or exclude one. They flag data quality issues that the GP should know about before the consultation starts.
Why does response validity matter clinically?
Adults completing ADHD screening questionnaires can produce unreliable data for several distinct reasons, none of which implies intent to deceive.
Under-reporting is well-documented in the clinical literature. Adults with longstanding undiagnosed ADHD have often developed compensatory strategies over decades. What they experience as normal effort, others experience as unusual difficulty. They underestimate their symptoms because their baseline has shifted. The AADPA Clinical Practice Guideline (2022) identifies this pattern and notes that collateral information from a partner, family member, or close associate is an important component of a thorough adult ADHD assessment. This is partly because the patient themselves cannot always see what others see.
Over-reporting is also common, and again, rarely intentional. A patient who has spent months researching ADHD before seeking assessment, who is afraid of being dismissed or not believed, may answer every symptom at maximum severity regardless of actual day-to-day frequency. Research by Becke et al. (2021) identified non-credible symptom reporting in clinical ADHD evaluations as a meaningful source of data quality concern, separate from deliberate fabrication (Journal of Neural Transmission).
A third category is inattentive completion: rushing through questions, answering without reading, treating the questionnaire as an obstacle to get through rather than a clinical instrument. This produces data that reflects completion behaviour, not symptom experience.
The GP reviewing a clinical summary without any validity information is working with data of unknown quality. Response validity signals change that.
What are the five signals in Velluto’s validity model?
Velluto checks five signals automatically as part of the clinical preparation process. All five are deterministic and rule-based. No AI is involved. The logic is transparent and independently verifiable by the GP.
Each signal produces one of four ratings: OK, REVIEW, CONCERN, or NOT APPLICABLE. OK means the data fell within typical patterns for the signal. REVIEW means the data warrants clinical attention. CONCERN means the pattern is stronger and warrants closer exploration. NOT APPLICABLE is used when the data needed for the check is not available (for example, V4 when no observer was nominated, or V3 when timing data is missing). The GP sees the underlying data behind every rating, not just the label.
This matters for regulatory and clinical reasons. The TGA’s February 2026 guidance confirms that glass-box systems are eligible for the Clinical Decision Support Software exemption. Glass-box means a clinician can verify the basis of each output. AI-based systems are not eligible. Velluto’s validity model is glass-box: for each signal, the GP can see exactly what triggered a rating and why.
Signal 1: Self-report consistency
Velluto’s ASRS implementation includes six validation question pairs. Each validation question is paired with a specific ASRS item, but appears separately in the questionnaire, randomised so it is never adjacent to its paired item.
When a patient answers the ASRS item and its validation counterpart, those answers should be broadly consistent. A pair counts as inconsistent when the ASRS score and the paired validation score differ by 2 or more points on the 0 to 4 scale. If a patient rates an item as highly frequent on the ASRS side and the same domain as rare or absent on the paired validation question, that pair is counted.
Two inconsistent pairs out of six produces a REVIEW rating. Three or more produces a CONCERN rating. The signal reports the exact number of inconsistent pairs in the summary so the GP can see the magnitude.
This design requires the patient to read and consider each question independently. It cannot be gamed by answering a template, because the template would produce inconsistencies. It also catches genuinely confused responders: patients who did not understand a question and answered inconsistently without realising it.
Signal 2: Severity distribution
Clinical presentations of ADHD produce characteristic answer patterns. Genuine moderate-to-severe ADHD self-reports typically show a mix of high, medium, and lower-rated items. Near-uniform patterns at maximum severity are uncommon.
Signal 2 counts how many of the 18 ASRS items were rated at the maximum score (4). When more than 80 percent of items (15 or more of 18) are at maximum, the signal is rated REVIEW. When more than 95 percent (effectively 18 of 18) are at maximum, it is rated CONCERN.
The signal does not interpret the clinical meaning of the scores. It flags the pattern for the GP to probe. A genuine severe ADHD presentation may trigger a REVIEW rating. That is acceptable: the rating is not a verdict, it is a prompt for clinical attention.
Signal 3: Completion speed
Velluto records the total time the patient spent completing the questionnaire and divides it by the number of items shown, producing an average seconds-per-item figure.
When the average time per item falls below 4 seconds, Signal 3 is rated CONCERN. Four seconds is the threshold below which most patients have not read the question before selecting an answer. The GP sees the actual seconds-per-item figure in the summary, not just a rating.
This catches a specific failure mode: the patient who opens the questionnaire at 11pm the night before their appointment, is tired or distracted, and taps through every question without reading it. The answers may look like plausible ADHD data. The completion time reveals they were not.
Signal 3 is rated NOT APPLICABLE when timing data is missing, for example if the assessment was completed across an unusually long span and the recorded duration does not reflect active engagement time.
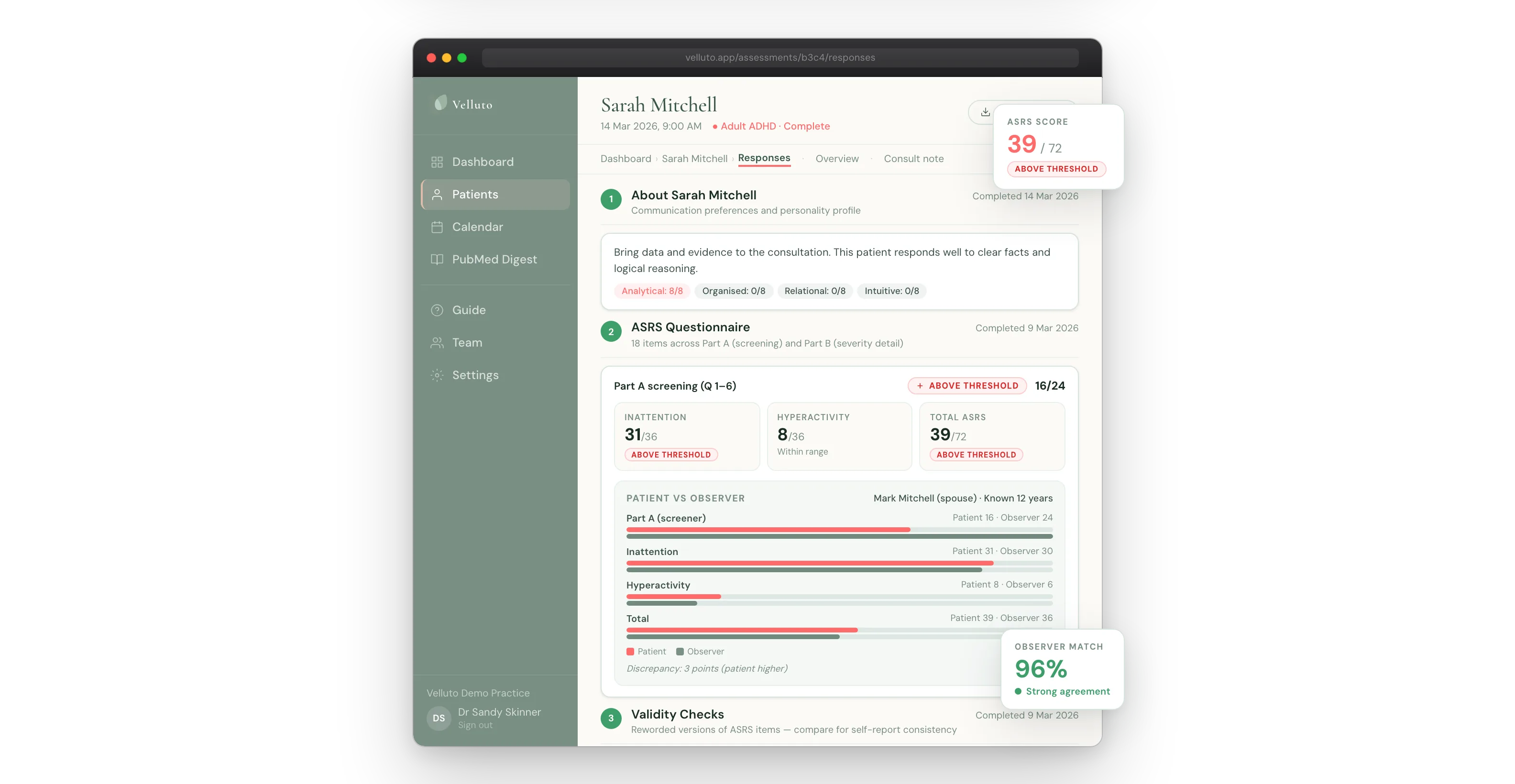
Signal 4: Self-report vs observer agreement
When a patient nominates an observer (a partner, parent, or employer who completes their own questionnaire about the patient’s symptoms), Velluto compares the two data sets.
Self-report and observer scores do not always agree. As the observer workflow article on this site discusses, discrepancy is expected and clinically informative in both directions. Signal 4 is not triggered by any discrepancy: it is triggered only when the gap is large enough to fall outside the typical range.
The signal calculates the absolute difference between the patient’s ASRS total and the observer’s total. The ASRS total is out of 72. A difference greater than 20 points produces a REVIEW rating. A difference greater than 35 points produces a CONCERN rating.
When the signal fires, the GP sees both totals, the absolute difference, and the direction of the gap (patient rating higher, or observer rating higher). The clinical interpretation remains the GP’s.
For paediatric assessments, this signal compares parent and teacher reports rather than self-report and observer, since the patient is a child and parent-teacher agreement is the equivalent data quality check.
Signal 4 is rated NOT APPLICABLE when no observer was nominated.
Signal 5: Childhood onset consistency
DSM-5 requires that ADHD symptoms were present before age 12. Velluto’s adult intake includes a childhood self-report section asking the patient to describe their experience during primary school and secondary school. This section is distinct from a direct question about age of onset.
Signal 5 compares the stated age of symptom onset with what the patient reports about their childhood experiences. When a patient states onset after age 12 but their childhood self-report describes significant primary-school difficulties with attention and organisation, that inconsistency is flagged.
The reverse also applies: a patient who states childhood onset but reports no difficulties before the age of 18 in the self-report section produces a signal worth exploring.
This applies to adult assessments only.
How should a GP interpret validity signals?
Validity signal ratings indicate that the data in one or more signals warrants additional attention before or during the clinical interview. They do not produce a finding. They do not indicate ADHD or exclude it.
A REVIEW rating means the data pattern warrants clinical attention. A CONCERN rating signals a stronger pattern that warrants closer exploration. Neither rating constitutes a clinical finding. Both are prompts for the GP to probe.
A useful frame is to read validity ratings the way you would read a discrepancy between two blood test results: something to note, explore, and factor into your clinical judgement. The rating tells you the data has a quality issue. You decide what to do with that.
Practically, a CONCERN rating on completion speed might prompt the GP to verbally re-run two or three key ASRS items in the consultation. A REVIEW rating on severity distribution might prompt a more detailed conversation about specific symptom domains. A REVIEW or CONCERN on self-report vs observer might prompt exploration of which settings the observer has seen the patient in and which they have not.
When multiple signals are rated REVIEW or CONCERN simultaneously, the GP has stronger grounds to explore the data quality issues in depth. When all signals are rated OK, the GP has higher confidence that the self-reported data reflects the patient’s genuine experience.
The clinical summary pack shows the validity signal results clearly. Five OK ratings are documented the same way as three CONCERNs: the GP sees the status of each signal before the consultation.
Is a validity rating the same as malingering or symptom fabrication?
No. A validity rating is a data quality indicator. It does not assert that the patient is being dishonest, that they are feigning symptoms, or that they have an ulterior motive.
This distinction matters clinically and ethically. The research literature distinguishes between noncredible responding and deliberate fabrication: Suhr and Berry (2017) note that invalid symptom reporting in ADHD evaluations can arise from multiple sources, including genuine confusion, heightened anxiety about assessment outcomes, prior coaching, or inattentive completion. None of these require any deceptive intent.
Velluto’s validity model is framed exactly this way. The ratings identify patterns in the data. The GP has the clinical context, the relationship with the patient, and the skills to probe what those patterns mean. The system presents patterns. The GP interprets them.
Patients never see the validity results. The summary pack is GP-only information. This is a deliberate design decision: presenting validity flags to patients would serve no clinical purpose and has real potential to damage the therapeutic relationship before the consultation has started.
The voice DNA document governing all Velluto GP-facing content is explicit about this: never use the words malingering, faking, suspicious, or drug-seeking. This applies to patient-facing copy and GP-facing copy alike. The validity model sits within that frame.
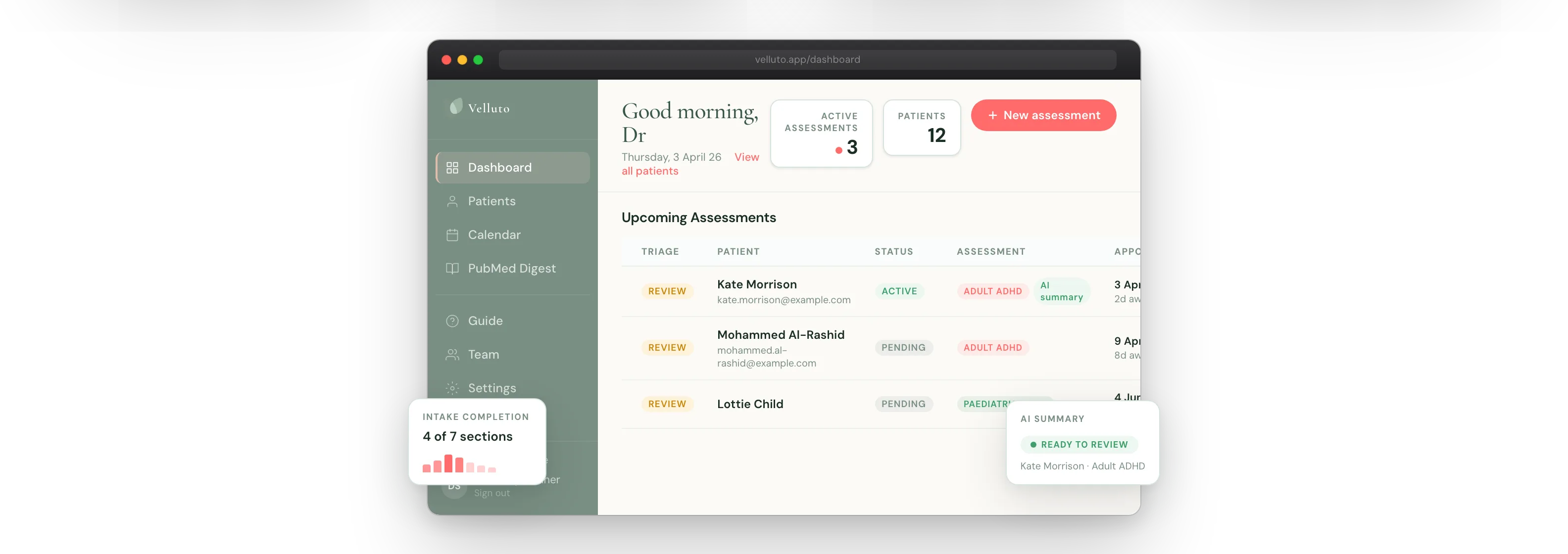
What does Velluto actually do with the five signals?
When a patient completes their pre-appointment intake, Velluto runs all five signals automatically. No additional steps are required from the GP or the practice.
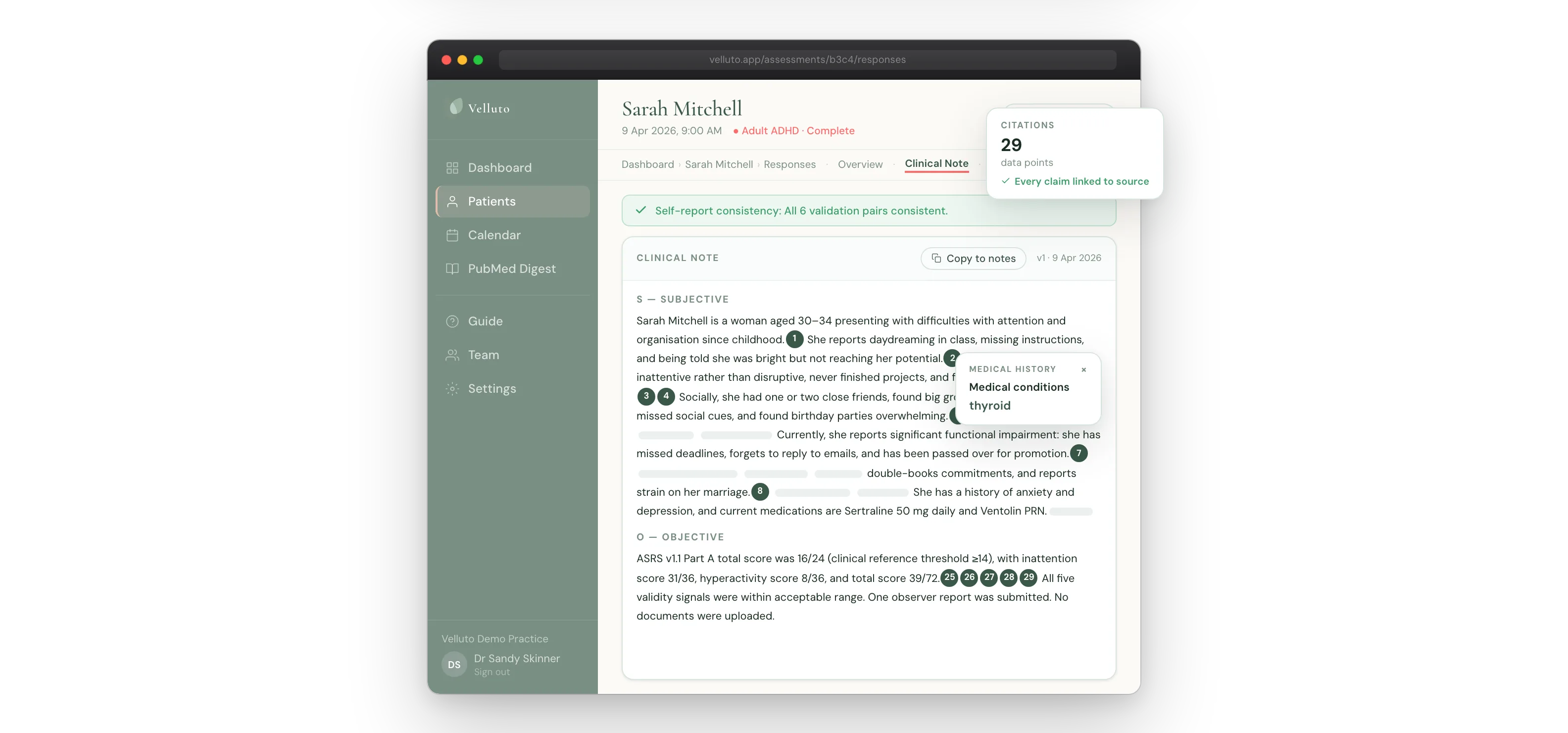
The results appear in the clinical summary pack the GP reviews before the consultation. The validity section of the pack shows:
- The rating of each signal (OK, REVIEW, CONCERN, or NOT APPLICABLE)
- For signals rated REVIEW or CONCERN: the specific data that produced the rating (e.g. “Average response time was 2.4 seconds per item, faster than typical”)
- For the self-report consistency signal: how many of the six validation pairs were inconsistent
- For the severity distribution signal: how many of the 18 items were rated at maximum severity, and the percentage
- For the self-report vs observer signal: both total scores, the absolute difference, and the direction of the gap
Where no observer was nominated, Signal 4 is rated NOT APPLICABLE, not as a flag.
The validity results are part of the clinical summary pack but are clearly separated from the scored questionnaire results. The GP can see the ASRS scores alongside the validity context, rather than seeing scores in isolation.
No other intake tool currently available in the Australian market checks all five of these signals automatically as part of standard clinical preparation. Paper ASRS forms cannot check completion speed. Without a digital observer workflow, the self-report vs observer signal cannot run. Without paired validation questions embedded in the questionnaire itself, internal consistency checking is not possible.
Self-reported ADHD data is the starting point for a GP-led assessment. Its quality varies. Completion speed, answer consistency, severity distribution, observer agreement, and childhood onset consistency each capture a different dimension of that quality, and each can fire independently of the others.
A clinical summary with validity signals gives the GP more to work with before the first question is asked. The GP still decides what to do with that information. What changes is whether the GP is walking into the consultation knowing the data quality, or finding out through the clinical interview.
Related in this series
Companion posts on how Velluto prepares the evidence before an ADHD consultation.
ASRS v1.1 questionnaire: what GPs need to know about administering it properly
Proper administration of the ASRS v1.1 in general practice, and what digital delivery changes.
Observer reports in GP ADHD assessment: what they are and why they change the consultation
How observer reports change the quality of evidence before the consultation.
Childhood school reports in adult ADHD assessment
Using school reports and developmental records as childhood onset evidence in adult ADHD assessment.
What a GP receives before an ADHD consultation with Velluto
What a GP receives before an ADHD consultation, scored and cross-referenced.
Frequently asked questions
What is response validity in ADHD assessment?
Response validity in ADHD assessment refers to whether a patient’s self-reported symptom data is a reliable reflection of their actual experience. It is distinct from diagnostic validity: response validity evaluates the quality of the data itself, before clinical interpretation. A response validity check asks whether the patient read and considered each question, whether their answers are internally consistent, and whether the overall pattern is clinically plausible.
Why do ADHD self-report questionnaires need validity checking?
Adults completing ADHD screening questionnaires produce unreliable data for several documented reasons, none of which require deceptive intent. Long-established compensatory strategies lead some patients to underestimate their symptoms. Fear of not being believed leads others to answer at maximum severity regardless of actual frequency. Tired or distracted completion produces data that reflects the conditions of completion, not the patient’s symptom experience. Without a validity check, the GP has no way of knowing which category applies to the data they are reviewing.
What are the five signals Velluto checks for response validity?
Velluto checks: (1) self-report consistency, whether paired validation questions match their corresponding ASRS items (REVIEW when 2 of 6 pairs differ by 2 or more points, CONCERN when 3 or more do); (2) severity distribution, the percentage of items rated at maximum severity (REVIEW above 80 percent, CONCERN above 95 percent); (3) completion speed, the average seconds per item (CONCERN when below 4 seconds); (4) self-report vs observer agreement, the absolute difference between patient and observer totals (REVIEW above 20 points, CONCERN above 35 points); and (5) childhood onset consistency, whether stated age of onset matches the childhood self-report. Each signal is rated OK, REVIEW, CONCERN, or NOT APPLICABLE. All five signals are deterministic and rule-based. No AI is involved.
Does a validity rating of REVIEW or CONCERN mean the patient is lying or faking ADHD?
No. A validity rating is a data quality indicator, not an accusation. Research distinguishes noncredible responding from deliberate fabrication: invalid symptom reporting in ADHD evaluations frequently arises from anxiety about the assessment process, prior coaching, confusion about question wording, or inattentive completion. None of these involve deceptive intent. Validity ratings identify patterns the GP should explore in conversation. The GP determines the clinical significance.
Do patients see their validity results in Velluto?
No. Validity results are GP-only information. They appear in the clinical summary pack that the GP reviews before the consultation, but patients do not have access to them. This is a deliberate design decision: validity ratings are clinical data quality indicators for the GP, not information that serves any purpose for the patient.
Are Velluto’s validity signals AI-based?
No. All five validity signals are deterministic and rule-based. The regulatory literature calls these glass-box systems. The logic is transparent, documented, and independently verifiable by the GP. This matters for TGA regulatory positioning: the TGA’s February 2026 guidance on clinical decision support software confirms that glass-box systems are eligible for the CDSS exemption, while AI-based systems are not.
How does a GP use validity rating information in a consultation?
Validity ratings tell the GP that one or more aspects of the self-reported data warrant additional attention. In practice, a CONCERN on completion speed might prompt verbal re-administration of key ASRS items during the clinical interview. A REVIEW or CONCERN on self-report vs observer might prompt exploration of which settings the observer has seen the patient in. A REVIEW on paired validation questions might prompt the GP to ask those specific items directly. The ratings do not change the clinical pathway. They inform how the GP probes the data.
Clinical information disclaimer
This article contains general clinical information for healthcare professionals. It is not a substitute for individual clinical judgement, professional guidelines, or specific patient assessment. Always apply your own clinical reasoning when making treatment decisions.
Velluto is a clinical intake platform. It does not diagnose, recommend treatment, or make clinical decisions. All clinical decisions remain with the treating GP.