The DSM-5 requires that “several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years.” It does not require a diagnosis before age 12. It does not require a formal assessment in childhood. It requires symptoms. Some form of evidence that those symptoms existed is needed.
Quick links
- At a glance
- What does the DSM-5 require regarding childhood onset of ADHD?
- What counts as evidence of childhood symptoms?
- Why are school reports clinically useful?
- What do you do when the patient has no school reports?
- What alternative evidence is acceptable?
- How should GPs evaluate the quality and consistency of retrospective evidence?
- What does digital document upload and AI extraction change about this step?
- What does Velluto do with supporting documents?
- Frequently asked questions
At a glance
| Component | Detail |
|---|---|
| DSM-5 criterion | Several symptoms present prior to age 12 years |
| What it requires | Evidence of symptoms, not a childhood diagnosis |
| Best documentary evidence | School reports (teacher comments on attention, behaviour, work completion) |
| Other acceptable evidence | Developmental records, parent report, NAPLAN or standardised test history, early childhood health records |
| When nothing exists | Document the attempt, record patient and informant recollection, note limitations |
| Reliability of recall | Adult self-recall of childhood ADHD symptoms has limited accuracy (Breda et al., 2020: 55.4% overall accuracy) |
| What Velluto does | AI extracts key phrases from uploaded documents; GP reviews the extraction |
What does the DSM-5 require regarding childhood onset of ADHD?
The DSM-5 Criterion D for ADHD states: “Several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years.”
Three things matter in the exact wording.
“Several” means more than one. The criterion does not specify how many, but it is more than an isolated teacher complaint. The broader symptom picture needs to support a history of difficulties that pre-date age 12.
“Prior to age 12” is not a diagnostic age. Many adults now presenting for assessment were children in the 1980s and 1990s, before ADHD was routinely assessed in Australian primary schools. The absence of a childhood diagnosis is not evidence against ADHD. The criterion asks when symptoms were present, not when they were identified.
“Were present” allows retrospective evidence. The DSM-5 does not require contemporaneous documentation. A credible retrospective account from the patient, from a parent, or from teacher records is acceptable. The quality and consistency of that account is a clinical judgement.
What the criterion does not allow is a diagnosis based purely on current adult presentation with no childhood onset evidence whatsoever. If a patient reports that all their difficulties began in their mid-30s with no earlier history, that pattern warrants careful clinical consideration before meeting Criterion D.
What counts as evidence of childhood symptoms?
Evidence exists on a spectrum from contemporaneous documentary records to unverified retrospective recall. More weight attaches to evidence collected closer to the time, from an independent observer, in a structured format.
School reports sit at the strongest end of the documentary spectrum. A school report is a contemporaneous account written by a teacher who observed the child across an extended period in a structured setting. Teacher comments on attention, focus, organisation, task completion, and classroom behaviour are highly relevant. Even neutral language such as “could try harder,” “has difficulty settling,” “loses focus during independent work” describes the same construct the GP is assessing in adult form.
Developmental records include health records from early childhood (MCHN notes, GP records from childhood, paediatrician letters), hospital records, and any formal assessments carried out in primary or secondary school (speech pathology, learning support, occupational therapy).
Standardised test and programme history: NAPLAN score reports and narrative comments, reading intervention programme records, or gifted and talented assessment reports can support a childhood profile even where direct ADHD assessment did not occur.
Parent recollection is an informant report, not a documentary record. It carries more weight than patient self-recollection because the informant observed the child as an external party. It carries less weight than contemporaneous documentation. It is still clinically useful, particularly when parents can describe specific situations, settings, and patterns, not just a general impression.
Why are school reports clinically useful?
School reports provide something that adult self-report cannot: an external, contemporaneous observation of the child in a setting specifically designed to challenge attention, behavioural regulation, and executive function.
School is, in clinical terms, an ideal ADHD diagnostic environment. It requires sustained attention, task completion, impulse control, organisation, and compliance with delayed gratification over an extended period every weekday. Teacher reports from this setting capture behaviour that is structurally related to the DSM-5 inattention and hyperactivity-impulsivity criteria.
A teacher who wrote in 1993 that a child “struggles to complete tasks independently, is often distracted by other students, and forgets to bring materials to class” was describing DSM-5 Criterion A items without knowing it. That observation, in a school report from age 8, is strong retrospective evidence of childhood onset.
School reports also carry a key advantage: they were not written for the purpose of supporting an ADHD assessment. They are independent, contemporaneous, and uninfluenced by the patient’s current belief about their own diagnosis.
What do you do when the patient has no school reports?
The absence of school reports is common. It does not make an assessment impossible. It changes what evidence is available and raises the bar on documentation of what was collected and what was not.
When school reports are not available, the options are:
Ask about where records might be. A patient who attended a single primary school may find that the school retains records, or that the local education authority holds archived records. Some Australian state education departments retain historical records. This is not always a practical avenue, particularly for older patients or those educated in other countries, but it is worth noting in the intake process.
Seek a parent informant report. If a parent is alive and accessible, their account of the patient’s childhood behaviour is the next strongest retrospective source. A structured informant questionnaire directed at childhood behaviour is more clinically useful than a verbal account in the consultation room. The AADPA Clinical Practice Guideline (2022) recommends including collateral information as part of a thorough adult ADHD assessment, and the principle applies equally to childhood onset evidence.
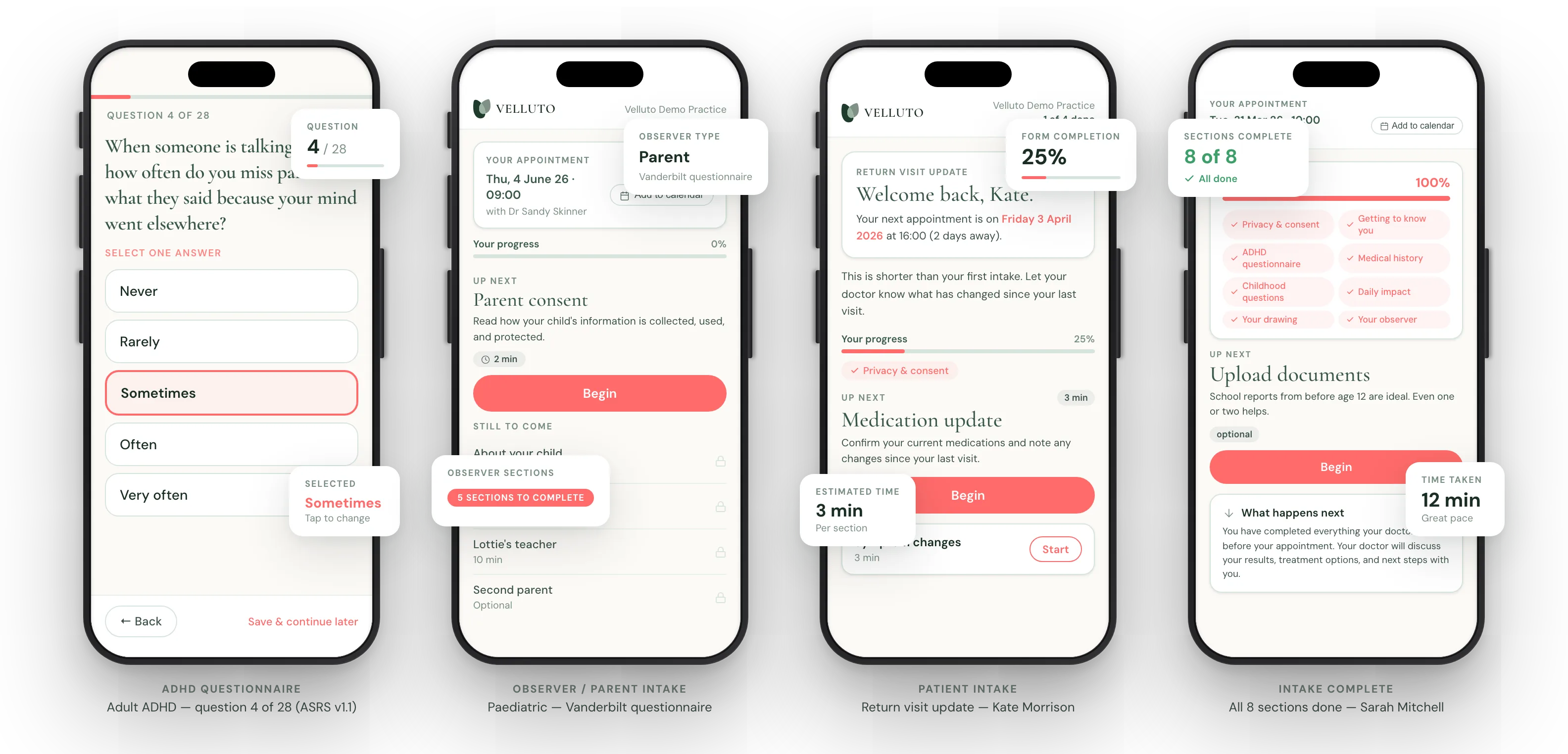
Collect structured patient self-report of childhood. Adult self-recall of childhood ADHD symptoms has known reliability limitations. Breda et al. (2020) found that retrospective self-reporting of childhood ADHD symptoms at age 22, compared against documented assessments from age 11, had an overall accuracy of only 55.4%, with sensitivity of 32.8% (Psychological Medicine, PMID 30968792). The direction of error matters: adults with current inattention symptoms tend to over-report childhood difficulties; others may under-report. Structured childhood self-report questionnaires that ask about specific settings and behaviours rather than general impressions produce more useful data than open-ended recall.
Document what was sought and not found. The absence of childhood records is clinically significant and should be recorded. A clinical summary that states “patient unable to locate school reports; attended X primary school, records not accessible; parent informant report obtained; childhood self-report completed” gives a future reviewer a clear picture of what evidence was available and how it was gathered. An unacknowledged absence is a gap. An acknowledged and documented absence, with alternative evidence recorded, is a reasonable clinical account.
What alternative evidence is acceptable?
Where school reports are unavailable, the following are recognised as relevant supporting evidence:
Developmental records (MCHN, GP, paediatric). Maternal and child health nurse records, childhood GP records, paediatric referral letters, and early childhood health assessments may document developmental concerns, referrals for behavioural concerns, or motor development patterns. These are contemporaneous records and carry weight.
Parent recollection of specific behaviours and settings. The most clinically useful parent accounts describe specific situations: “She was always called out for talking in class,” “He had to stay back after school every week because he couldn’t finish his work,” “The teacher rang us in Year 3 about her not sitting still.” Specific, situation-anchored accounts are more reliable than general impressions (“he was always hyperactive”).
NAPLAN and standardised test narratives. NAPLAN results themselves do not indicate ADHD. However, narrative comments attached to standardised tests, or a pattern of performance inconsistency across years, can form part of a childhood evidence profile when taken with other sources.
School intervention or support records. Records of enrolment in reading intervention programmes, learning support, occupational therapy referrals through school, or gifted/enrichment programmes may document a childhood profile even where ADHD was not named.
The clinical standard is not to have all of these. It is to collect what is available, document what is not, and make a clinical judgement about the weight and consistency of the evidence collected.
How should GPs evaluate the quality and consistency of retrospective evidence?
Not all retrospective evidence is equal. When reviewing childhood evidence, whether documentary or recalled, three questions are worth applying:
Is it independent? Evidence from a source independent of the patient (a teacher, a parent, a document written before the assessment process began) carries more weight than the patient’s own account of what they believe their childhood was like. Independence is what gives corroborating evidence its clinical value.
Is it specific? Vague general impressions (“she was always a handful”) are less useful than specific, observable behaviours (“he lost his homework so often the teacher gave up asking for it”). Specific accounts can be mapped against DSM-5 criteria. General impressions cannot.
Is it consistent with the current presentation? Where a patient’s current symptom profile, childhood self-report, and any informant account all describe the same core pattern of difficulties across settings and time, that consistency is clinically informative. Where they diverge significantly, the divergence is worth exploring in the clinical interview.
The research literature adds context here. Breda et al. (2020) found that adults with current inattention symptoms showed higher rates of false-positive recall of childhood difficulties. This suggests that when a patient reports a very strong childhood history with no corroborating documentation, the clinical picture warrants careful review rather than uncritical acceptance. The GP is not adjudicating the patient’s honesty. They are assessing the quality and consistency of the evidence available, which is a different task.
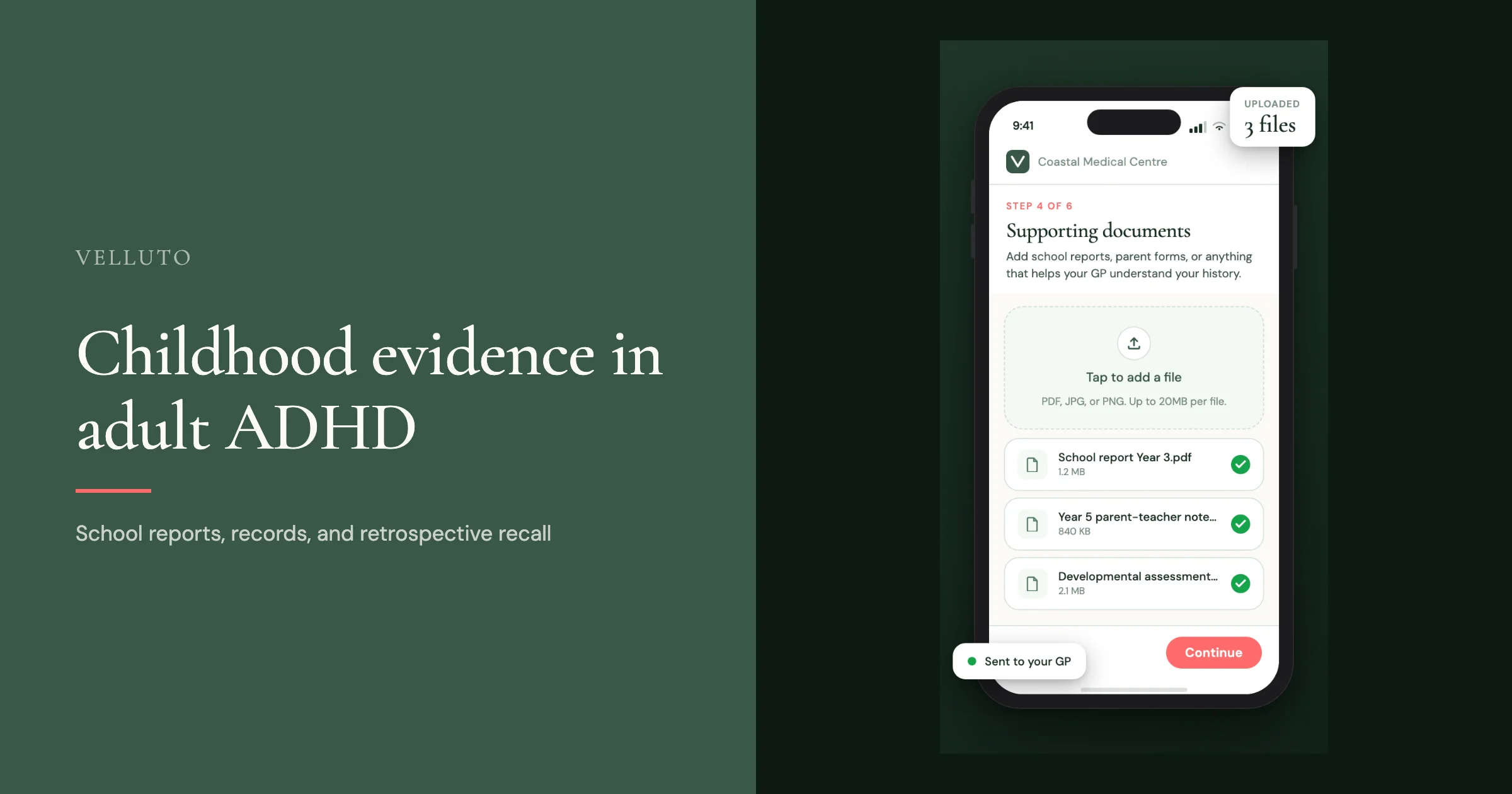
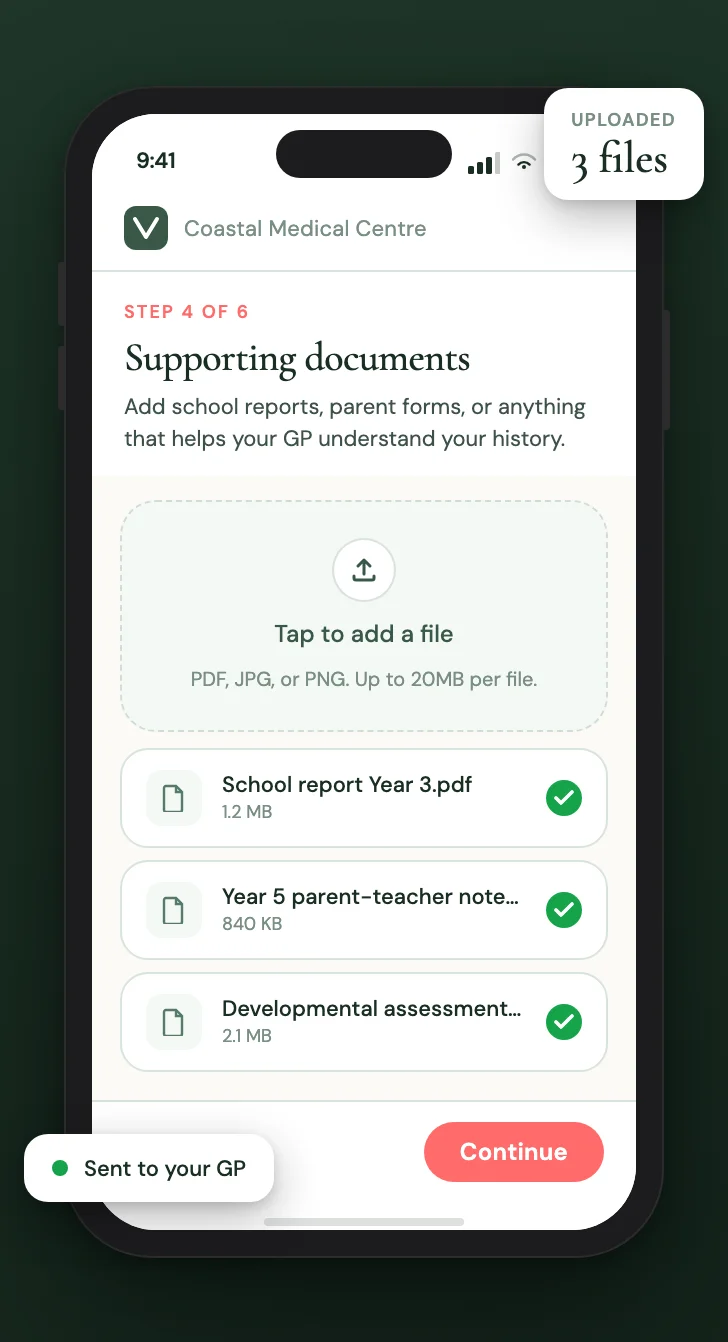
What does digital document upload and AI extraction change about this step?
Until recently, the school report step in an ADHD assessment looked like this: the GP asks the patient to bring any school reports they can find. The patient searches at home, perhaps asks their parents, finds some or nothing, and arrives at the appointment with whatever they managed to locate. The GP reads the reports during the consultation, identifies relevant teacher comments, and incorporates them into their clinical reasoning. This happens in 45 minutes, while also conducting the full clinical interview.
Digital document upload before the appointment changes the time equation. When a patient uploads school reports, historical records, or developmental documents as part of their pre-appointment intake, those documents are available to the GP before the consultation begins. The GP is not reading reports in the room. They are reviewing a prepared extraction.
This matters particularly because the relevant content in a school report is often a small fraction of the document: one or two teacher comments on a page of handwriting assessments and reading levels. Without structure, finding those comments requires reading the whole document.

What does Velluto do with supporting documents?
When a patient uploads documents through their Velluto intake, each document is processed by Velluto’s AI document extraction pipeline. The model (Gemini 2.5 Flash, hosted in Australia at Google’s australia-southeast1 region) reads the document and extracts:
- Key findings relevant to the assessment
- Approximate date and the patient’s approximate age at the time
- Any prior diagnoses or interventions mentioned
- A confidence level for the extraction
- The full extracted text
Patient data is de-identified before being sent to the AI provider. Patient names, GP names, and practice names are replaced with tokens before the API call. No patient data is used to train AI models. All AI infrastructure is hosted in Australia.
The extraction appears in the GP’s clinical summary pack under “Childhood Evidence Summary”: key phrases from uploaded school reports, organised chronologically. The GP reviews the extraction alongside the raw documents, which remain accessible for the full consultation. The extraction is a reading aid, not a clinical interpretation. What the documents mean clinically is the GP’s assessment.
If no documents were uploaded, that is visible in the summary pack and in the readiness score (Green / Amber / Red). The absence is documented rather than invisible.
The DSM-5 childhood onset criterion asks a reasonable clinical question: was this a lifelong pattern or did it emerge in adulthood? The evidence available to answer that question varies widely depending on the patient’s age, background, and family circumstances.
School reports, when they exist, are the most useful single source. When they do not exist, a combination of parent informant report, developmental records, and structured childhood self-report provides a reasonable evidence base, provided the absence is documented and the limitations acknowledged.
The time cost of assembling this evidence before the consultation has historically made it the component most likely to arrive incomplete. Digital document upload, AI extraction, and structured childhood self-report sections in pre-appointment intake do not change what counts as acceptable evidence. They change how much of it is assembled and reviewed before the consultation begins.
Related in this series
Companion posts on how Velluto prepares the evidence before an ADHD consultation.
ASRS v1.1 questionnaire: what GPs need to know about administering it properly
Proper administration of the ASRS v1.1 in general practice, and what digital delivery changes.
Observer reports in GP ADHD assessment: what they are and why they change the consultation
How observer reports change the quality of evidence before the consultation.
Response validity in ADHD screening: the five-signal model
The five deterministic signals Velluto checks to flag data quality issues.

What a GP receives before an ADHD consultation with Velluto
What a GP receives before an ADHD consultation, scored and cross-referenced.
Frequently asked questions
What does the DSM-5 require for childhood onset of ADHD in adults?
The DSM-5 Criterion D requires that “several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years.” This is not a requirement for a childhood diagnosis, nor for a formal assessment in childhood. It requires evidence that symptoms existed before age 12. Acceptable evidence includes contemporaneous records such as school reports, developmental records, parent informant accounts, and structured patient self-report of childhood behaviour.
Are school reports required for an adult ADHD assessment in Australia?
School reports are not legally required for an adult ADHD assessment. They are the most useful form of documentary evidence of childhood onset because they are contemporaneous, written by an independent observer in a structured setting. When they are available, they carry significant clinical weight. When they are not available, the absence should be documented and alternative evidence sought, including parent informant reports, developmental records, and structured childhood self-report.
What do teacher comments in school reports show about ADHD?
Teacher comments in school reports describe classroom behaviour observed over an extended period in a setting that requires sustained attention, task completion, and impulse control. These are exactly the domains assessed by DSM-5 ADHD criteria. Comments such as “struggles to complete work independently,” “is often distracted,” or “has difficulty staying on task” describe Criterion A items without using clinical language. These are highly relevant retrospective evidence of childhood symptom onset.
How reliable is adult self-recall of childhood ADHD symptoms?
Adult self-recall of childhood ADHD symptoms has known reliability limitations. Breda et al. (2020) found that retrospective self-report of childhood ADHD symptoms had an overall accuracy of only 55.4% when compared against documented assessments (Psychological Medicine, PMID 30968792). Adults with current inattention symptoms tend to over-report childhood difficulties. This is why corroborating evidence from independent sources such as school reports, developmental records, and parent accounts is clinically important, and why the absence of corroboration is worth noting rather than ignoring.
What alternative evidence is acceptable when school reports don’t exist?
When school reports are unavailable, acceptable alternative evidence includes: parent informant accounts of specific childhood behaviours (more useful when tied to specific situations and settings); developmental records from maternal and child health nurses, childhood GPs, or paediatricians; NAPLAN narrative comments or other standardised test records; school intervention or learning support records; and, less commonly, accounts from older siblings. The clinical standard is to collect what is available, document what was sought but not found, and note the limitations of the evidence gathered.
Does not having school reports mean an adult ADHD assessment cannot proceed?
No. The absence of school reports does not make an adult ADHD assessment impossible. It changes the evidence profile. A GP can proceed with an assessment when school reports are unavailable, provided they collect whatever alternative evidence is available, document the absence of records and what was done to seek them, and make a clinical judgement about the weight and consistency of the evidence collected. The absence of corroboration is clinically relevant and should be recorded.
What does Velluto do with school reports uploaded by patients?
When a patient uploads school reports or other documents through their Velluto intake, Velluto’s AI extraction pipeline reads each document and extracts key findings, approximate dates, the patient’s approximate age at the time, and any prior diagnoses or interventions. Patient data is de-identified before processing, and all AI infrastructure is hosted in Australia. The extraction appears in the GP’s clinical summary pack under “Childhood Evidence Summary,” organised chronologically. The GP reviews the extraction alongside the original documents. All clinical interpretation is the GP’s.
Clinical information disclaimer
This article contains general clinical information for healthcare professionals. It is not a substitute for individual clinical judgement, professional guidelines, or specific patient assessment. Always apply your own clinical reasoning when making treatment decisions.
Velluto is a clinical intake platform. It does not diagnose, recommend treatment, or make clinical decisions. All clinical decisions remain with the treating GP.