An observer report is a structured questionnaire completed independently by someone who knows the patient well. A partner, parent, or sibling completes it, covering the same DSM-5 symptom criteria the patient answered about themselves, written in third-person format. It is not verbal feedback. It is not the patient’s account of what their partner thinks. It is independently collected, structured data from a person who has observed the patient across settings and over time.
Quick links
- At a glance
- What does an observer report collect?
- Why is self-report alone not sufficient for ADHD assessment?
- What do discrepancies between self-report and observer scores mean clinically?
- Is verbal collateral the same as an observer report?
- Why do paper observer forms fail in practice?
- How does digital delivery change the evidence available?
- What does Velluto do in this workflow?
- Frequently asked questions
At a glance
| Component | What it is |
|---|---|
| Observer questionnaire | 18 DSM-5 items in third-person format |
| Who completes it | Partner, parent, sibling, or employer |
| How it is collected | Independently, without patient involvement in the answers |
| What it adds | A second data point across different contexts |
| Discrepancy | Expected, clinically informative in both directions |
| Paediatric pathway | Two parents plus a teacher, using dedicated questionnaire forms |
What does an observer report collect?
An observer report covers the same DSM-5 inattention and hyperactivity-impulsivity criteria the patient answered, reframed for a third-person perspective. The observer is describing behaviour they have observed. They are not offering a clinical opinion, and not speculating about diagnosis.
The questionnaire collects:
- DSM-5 inattention and hyperactivity-impulsivity items, written for a third-person perspective
- Which settings the observer has seen these behaviours in, and over what timeframe
- The observer’s relationship to the patient
- A free-text section for anything outside the structured items
The observer’s perspective is independent. They have watched the patient over months or years, across contexts the GP will never see: at home, under deadline pressure, during the school run, in an unstructured weekend afternoon.
Why is self-report alone not sufficient for ADHD assessment?
Adults being assessed for ADHD often under-report symptoms. The mechanisms are well-documented in the clinical literature: long-developed compensatory strategies, normalisation of their own experience, difficulty distinguishing ADHD symptoms from their baseline, and genuine uncertainty about whether their internal experience is unusual. The AADPA Clinical Practice Guideline (2022) notes that collateral information from a partner, family member, or close associate is an important component of a thorough adult ADHD assessment.
Some adults over-report. They have researched the condition extensively and answer symptoms at maximum severity regardless of their actual day-to-day presentation. This is rarely intentional. It is usually anxiety about the process, or a fear of not being believed.
Self-report data is essential. It is also partial. It reflects what the patient believes about their own symptoms, filtered through their insight, their expectations, and the particular conditions of being assessed.
Observer data adds a second data point collected across different contexts, without the pressures of an assessment appointment. The observer is describing behaviour they have observed over time, not reporting how they feel right now.
What do discrepancies between self-report and observer scores mean clinically?
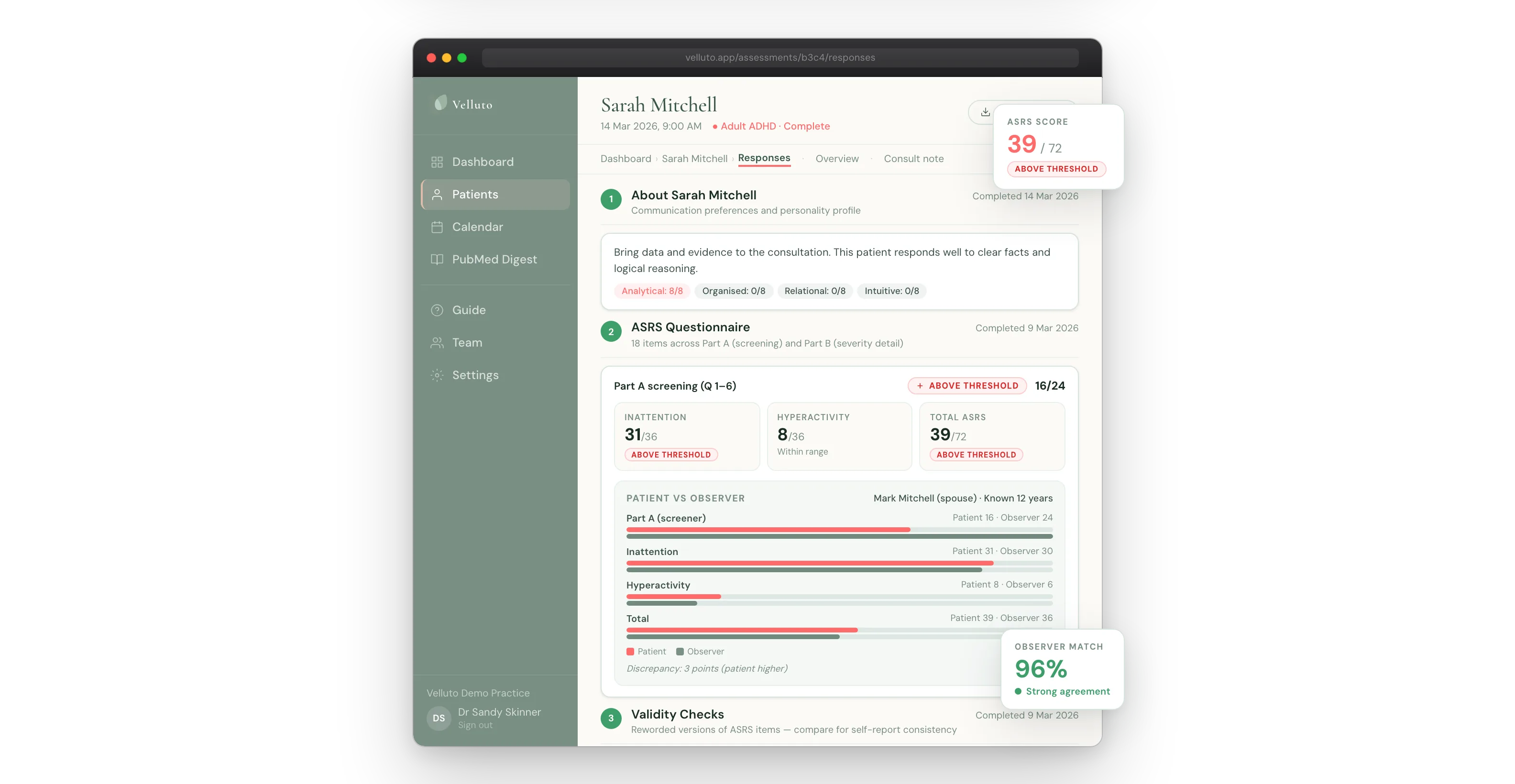
Self-report and observer scores do not match in a significant proportion of adult ADHD assessments. This is expected. The direction of the discrepancy is what matters clinically. The discrepancy itself is not the finding.
When the patient rates symptoms higher than the observer does, it often reflects that symptoms manifest in settings the observer does not see: at work, during solo tasks, or in the internal experience of executive function difficulty that does not produce externally visible behaviour. Compensatory strategies learned over years can mask symptoms from others while the internal load remains high. Worth exploring in the clinical interview.
When the observer rates symptoms higher than the patient does, it often reflects poor insight, well-developed strategies the patient no longer registers as effort, or a presentation that is more visible in its impact on others than on the patient’s own experience. Also worth clinical discussion.
Neither pattern constitutes a diagnostic finding on its own. Both are useful inputs into the clinical conversation. The GP decides what to make of them.
Is verbal collateral the same as an observer report?
No. Verbal collateral and a structured observer report are not equivalent.
Many GPs ask about collateral information during the appointment: “Have you spoken to anyone who knows you well about your symptoms?” The patient answers. The GP writes a note. That is not observer collateral.
A patient’s account of what their partner thinks is a filtered, secondhand report. The patient has already selected what to share, interpreted the partner’s words through their own frame, and recalled it during a clinical appointment. What reaches the GP is the patient’s self-report with an extra step.
The clinical value of observer collateral depends on the observer completing a structured questionnaire independently, without the patient’s involvement in how they answer. When the patient is the relay, the independence is lost.
Why do paper observer forms fail in practice?
Some practices hand the patient an observer form to take home. In theory this solves the problem. In practice, the form goes in a bag, gets lost, or sits on the kitchen bench for two weeks. The patient feels awkward asking their partner to fill it in. The partner fills it in but the patient forgets it on appointment day.
Even when a completed paper form does arrive, the GP still needs to score it manually, compare it to the self-report data, and document the comparison before the consultation. In a 45-minute appointment block, this rarely happens before the patient is already in the room.
The result: the GP planned on having observer data and does not have it. The absence is often invisible. It is not flagged anywhere, not factored into how the consultation is structured.
How does digital delivery change the evidence available?
When the observer questionnaire is sent directly to the observer, on their own device and at their own pace, several things change.
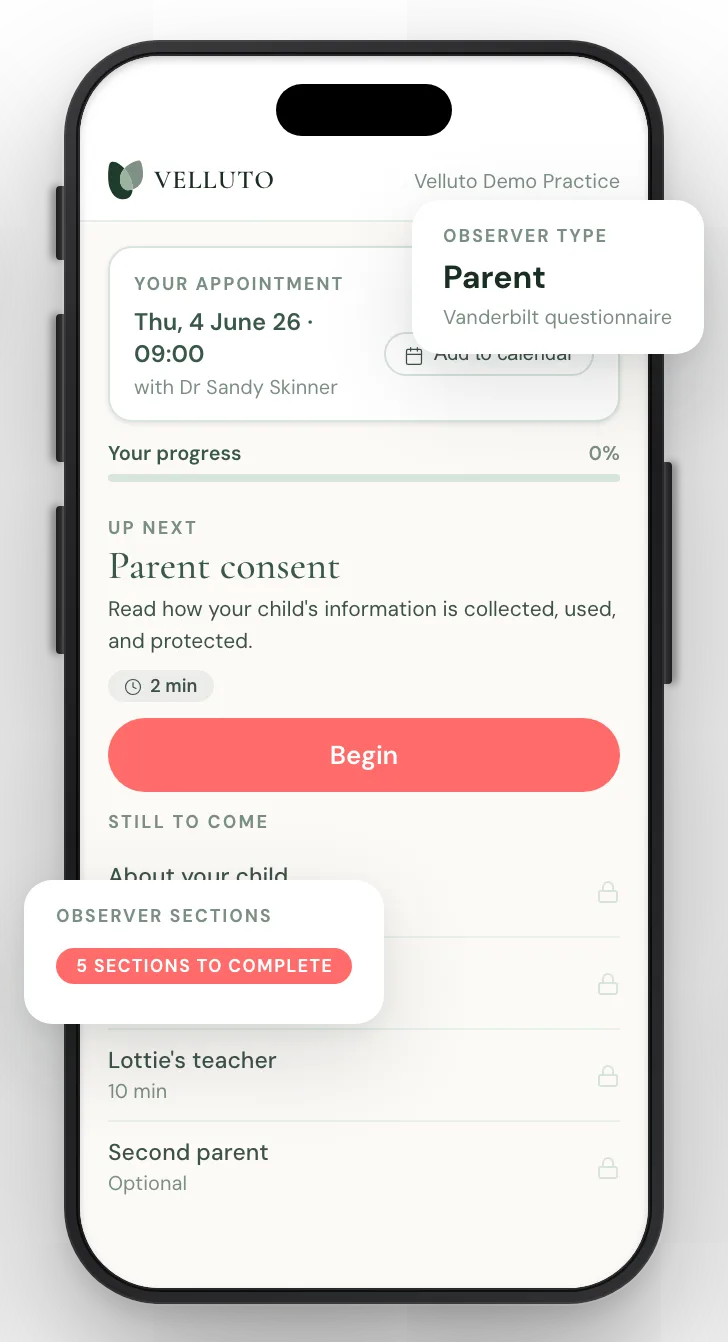
The patient nominates the observer during their pre-appointment intake. An invitation goes directly to that person. They complete the questionnaire independently, not in the patient’s presence, and not filtered through the patient’s account of what they should write. Automatic reminders follow if they have not completed it before the appointment.
The GP receives the observer report alongside the patient self-report, both scored, before the consultation begins. The discrepancy between them is visible. If no observer was nominated, that is visible too. It is documented in the clinical summary, not assumed to be absent for an unknown reason.
This changes the consultation from the first minute. The GP is not gathering information. They are reviewing it.
What does Velluto do in this workflow?
When a patient completes Velluto’s pre-appointment intake, they nominate up to two observers. Each observer receives a direct, secure link to their own questionnaire: 18 DSM-5 items in third-person format, plus a free-text section. The patient writes a personal message that is included in the invitation.
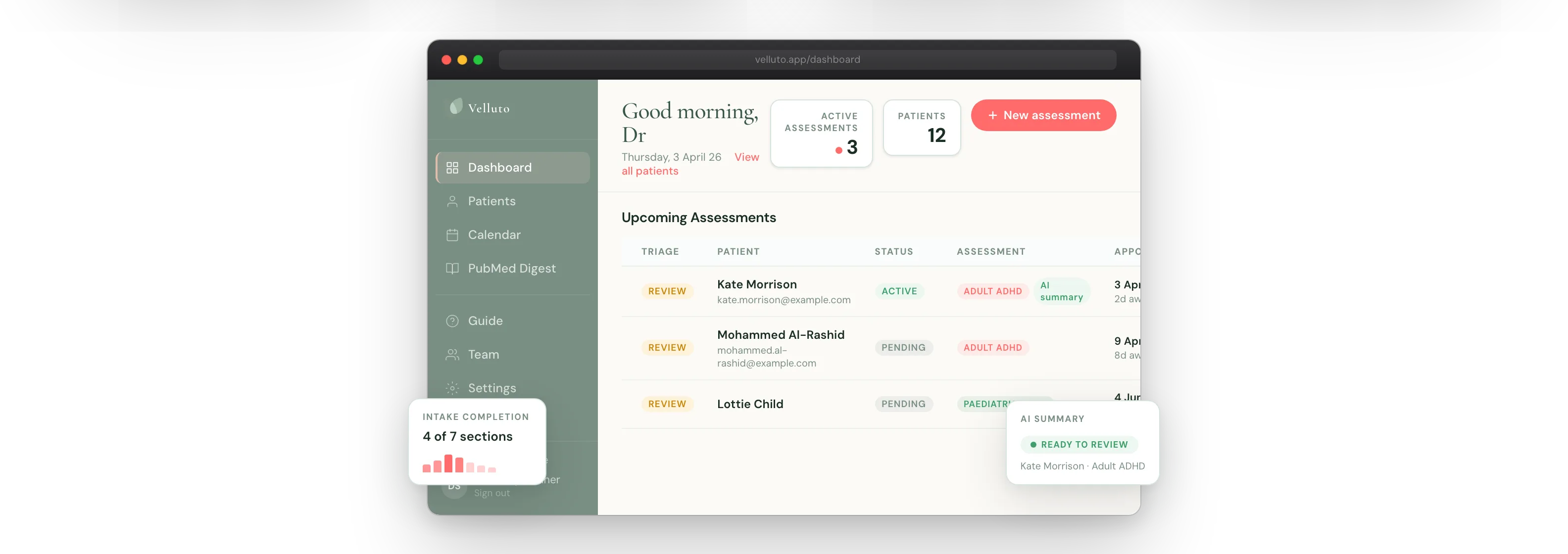
The patient sees real-time status for each observer on their intake checklist. The status shows Submitted or Waiting. The GP sees the same status on their dashboard.
If an observer has not completed by the appointment deadline, Velluto sends reminders automatically. The GP does not need to chase.
The observer report is included in the clinical summary pack the GP reviews before the consultation. Observer scores sit alongside patient self-report scores. Where discrepancy is present, it is flagged.
If no observer was nominated, the GP is notified in the summary. The clinical summary readiness score reflects whether this component is present: Green, Amber, or Red depending on what else is available.
For paediatric assessments, the observer pathway extends to two parents and a teacher, using dedicated parent and teacher questionnaire forms.
Most GPs want observer data. The practical barrier has never been the concept. It has been the process: a paper form that may or may not come back is not a reliable clinical input.
A questionnaire sent directly to the observer, completed independently, returned before the appointment, and scored alongside the patient self-report is a different instrument entirely. Not because the questions changed. Because the conditions under which it was collected changed.
Observer data gives the GP more to work with. What they do with it remains entirely their clinical judgement.
Related in this series
Companion posts on how Velluto prepares the evidence before an ADHD consultation.
ASRS v1.1 questionnaire: what GPs need to know about administering it properly
Proper administration of the ASRS v1.1 in general practice, and what digital delivery changes.
Childhood school reports in adult ADHD assessment
Using school reports and developmental records as childhood onset evidence in adult ADHD assessment.

Response validity in ADHD screening: the five-signal model
The five deterministic signals Velluto checks to flag data quality issues.
What a GP receives before an ADHD consultation with Velluto
What a GP receives before an ADHD consultation, scored and cross-referenced.
Frequently asked questions
What is an observer report in ADHD assessment?
An observer report is a structured questionnaire completed independently by someone who knows the patient well, typically a partner, parent, or sibling. It covers the same DSM-5 symptom criteria the patient answered, written in third-person format. The purpose is to provide a second data point from someone who has observed the patient across settings and over time.
Who should complete an observer report for an adult ADHD assessment?
The best observer is someone who knows the patient well and sees them regularly across different contexts. A partner, parent, sibling, or long-term employer are all appropriate. The observer should not be the patient’s treating clinician. The patient nominates the observer; the observer completes the questionnaire independently.
What is the difference between an observer report and verbal collateral?
Verbal collateral means asking the patient what their family or partner thinks of their symptoms. An observer report means the observer answers a structured questionnaire directly and independently, without the patient acting as relay. The two are not equivalent. When the patient is the relay, the independence is lost, and therefore so is the clinical value.
Do self-report and observer scores usually match in adult ADHD assessment?
No. Discrepancy between self-report and observer scores is common and expected in adult ADHD assessment. The direction of the discrepancy is clinically informative. When the patient rates symptoms higher than the observer, it may reflect internal symptoms or workplace presentations the observer does not see. When the observer rates symptoms higher, it may reflect poor insight or masking strategies the patient no longer registers as effort.
What does the AADPA guideline say about collateral information in ADHD assessment?
The AADPA Clinical Practice Guideline for ADHD (2022) identifies collateral information from a partner, family member, or close associate as an important component of a thorough adult ADHD assessment. The guideline notes the limitations of self-report alone given the well-documented patterns of under-reporting in adults with established compensatory strategies.
Is an observer report required for a GP-led adult ADHD assessment in Australia?
The AADPA CPG recommends collateral information as part of a thorough assessment; it is not a statutory requirement. Its absence is clinically relevant and worth documenting. A summary that includes observer data provides a richer clinical picture than one that does not.
How does Velluto collect observer reports?
When a patient completes their pre-appointment intake through Velluto, they nominate up to two observers. Each observer receives a direct invitation to complete an 18-item DSM-5 questionnaire independently, on their own device. The patient can include a personal message in the invitation. Automatic reminders are sent if the observer has not completed the questionnaire before the appointment. The scored results appear in the GP’s pre-consultation summary alongside the patient self-report.
Clinical information disclaimer
This article contains general clinical information for healthcare professionals. It is not a substitute for individual clinical judgement, professional guidelines, or specific patient assessment. Always apply your own clinical reasoning when making treatment decisions.
Velluto is a clinical intake platform. It does not diagnose, recommend treatment, or make clinical decisions. All clinical decisions remain with the treating GP.