Adult ADHD assessments are one of the most time-intensive consultation types in general practice — not because the diagnostic reasoning is difficult, but because the information gathering is. A GP who wants to do these assessments properly needs a reliable process for collecting patient questionnaires, observer reports, childhood evidence, and medical history before the appointment starts. Without that infrastructure, every assessment is an improvised data collection exercise in a 40-minute window.
This post covers the practical steps for setting up an ADHD assessment workflow in your practice: what the workflow needs to include, what tools are involved, and how to structure it so the consultation becomes clinical reasoning rather than form-filling.
Quick links
- What a complete workflow requires
- Step 1: booking and intake
- Step 2: observer reports
- Step 3: childhood evidence
- Step 4: the clinical summary
- Step 5: consultation and documentation
- Common workflow failures and how to avoid them
- Practice manager checklist
- Frequently asked questions
What a complete workflow requires
The AADPA Clinical Practice Guideline (2022) identifies five evidence components for a thorough adult ADHD assessment. A practice workflow needs to reliably collect all five before the consultation:
- ASRS v1.1 self-report — the validated 18-item questionnaire, plus subscale scoring
- Observer/collateral report — independently completed by a partner, parent, or sibling
- Childhood onset evidence — school reports, developmental records, or reliable parent recollection
- Medical and psychiatric history — to screen for differentials and co-occurring conditions
- Clinical interview — the consultation itself, which starts at the end of this list
Most of the work in this list happens before the patient walks in the door. The consultation is where you interpret, probe, and decide. The workflow is what gets you the evidence to interpret.
Step 1: booking and intake
When a patient books an ADHD assessment appointment, they should receive a structured intake link immediately. Not a PDF form. Not a phone call from reception asking them to bring documents on the day. A digital intake form they complete on their phone or computer before they arrive.
The intake should cover the ASRS v1.1 questionnaire, medical and mental health history, substance use, and basic demographics. It should be designed to take 25 to 35 minutes, split across multiple sittings if needed. Questions should appear one at a time — ADHD patients lose focus on long lists of checkboxes.
Automatic reminders should be sent if the intake is not completed within two to three days of the appointment. Reception staff should not need to chase patients manually.
What to avoid: sending patients a PDF to print, complete in the waiting room, and hand to reception. By the time the appointment starts, the GP has five minutes to read a handwritten form they have never seen before. That is not intake — it is theatre.
Step 2: observer reports
The observer report is the most commonly skipped step in GP ADHD assessments, and the one that makes the largest difference to the quality of the evidence available. An observer — a partner, parent, or sibling — completes an 18-item DSM-5 questionnaire independently, without the patient relaying their answers. The observer’s perspective covers contexts the GP will never see directly.
The workflow problem with observer reports is logistics. If you ask patients to “bring someone who knows you well” to the appointment, many cannot. If you give them a paper form to pass on, many lose it or forget. If you call the observer yourself, you have created a clinical administrative task that takes 15 minutes per patient.
The solution is to send the observer a direct digital invitation from the intake system. The patient nominates the observer’s name and email. The observer receives their own secure link, completes the questionnaire independently on their own device, and the scored results are available in the GP’s dashboard before the consultation. No paper. No phone calls. No chasing.
Step 3: childhood evidence
DSM-5 requires evidence that several inattention or hyperactivity-impulsivity symptoms were present before age 12. Establishing this in a 40-minute adult ADHD assessment without preparation is difficult. Most adults have no formal documentation. School reports exist in shoeboxes or parents’ attics. Some cannot contact their childhood school. Some were schooled interstate or overseas.
The workflow needs to ask patients to upload whatever childhood documentation they have before the appointment. The intake system should accept PDFs and photos. Any uploaded documents should be processed before the consultation, with key phrases extracted and organised for the GP’s review.
Where documents do not exist, the patient’s own childhood self-report and the observer’s account of long-term symptoms are the available evidence. The intake should collect this systematically, not as a live interview question in the appointment. A patient asked to recall childhood symptoms under time pressure in a clinical setting is not in ideal conditions for accurate recall.
Step 4: the clinical summary
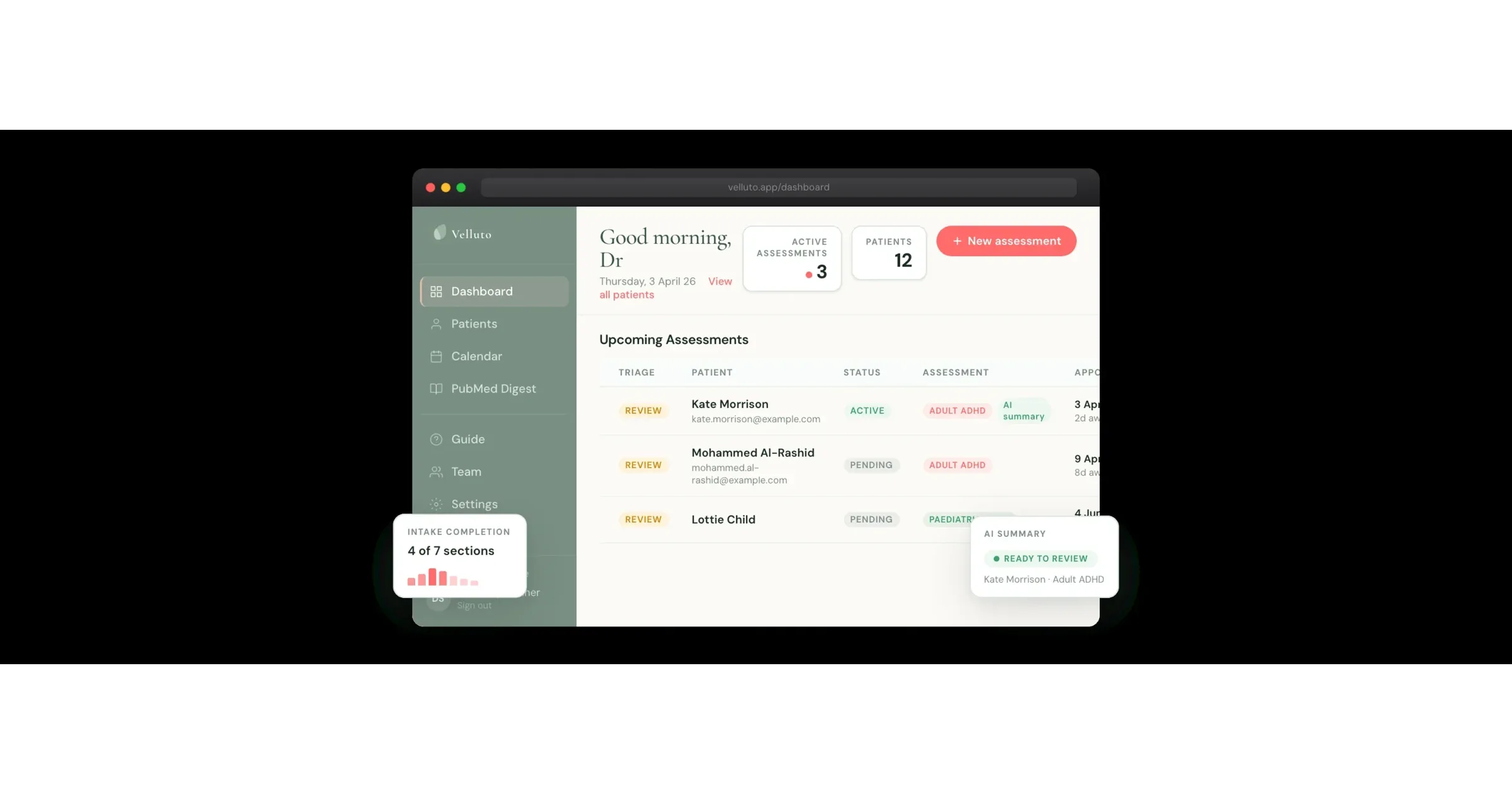
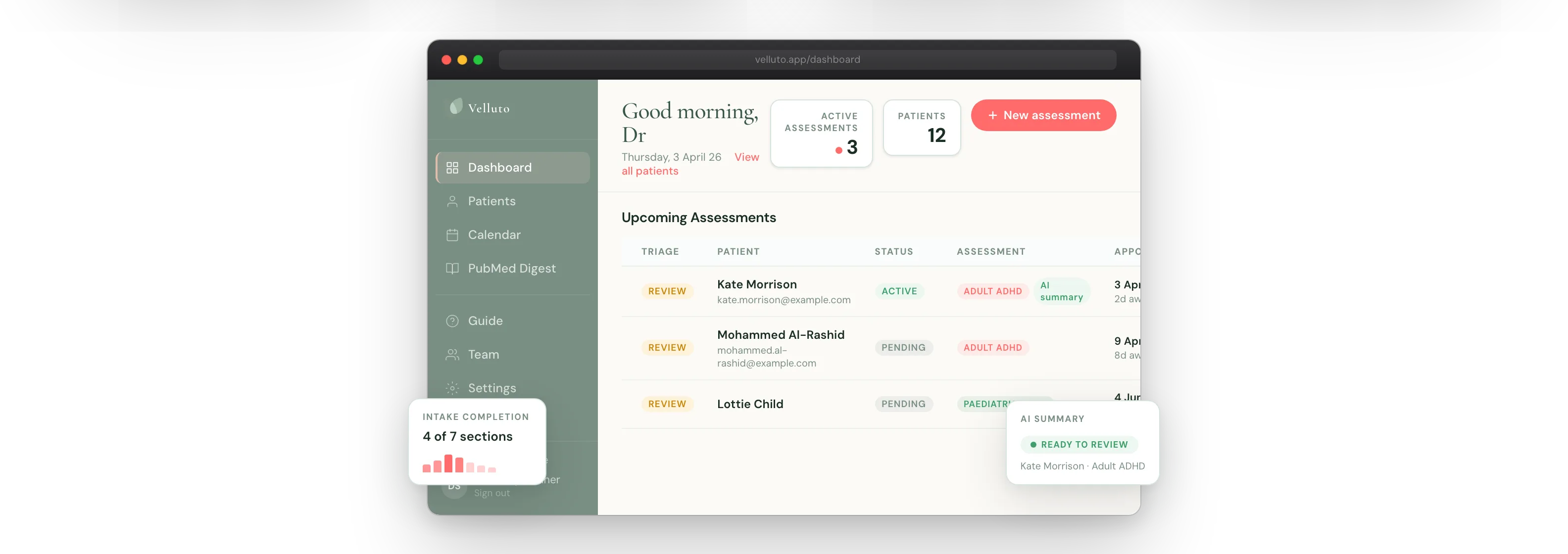
Everything collected in steps 1 to 3 needs to reach the GP in a usable form before the consultation starts. A pile of intake forms in a shared folder is not a clinical summary. A scored questionnaire, observer report, extracted childhood evidence, and a gaps report — assembled and ready to read in ten minutes — is.
The summary should include: ASRS subscale scores, observer report scores, key childhood evidence phrases, any inconsistency flags between data points, differential diagnosis flags based on the patient’s reported history, a gaps report listing anything incomplete, and a readiness indicator. Green means the consultation can proceed with full evidence. Amber means gaps exist but the consultation can still run. Red means critical evidence is missing and rescheduling should be considered.
The summary should be downloadable as a PDF for attachment to Best Practice or Medical Director. Clinical records need to contain the evidence, not just the clinical note.
Step 5: consultation and documentation
If the first four steps have been done well, the consultation is where the GP applies clinical judgement. You open the summary, review the scored data, identify the clinical questions that still need answering, and conduct the interview. You are not collecting information. You are interpreting it.
That shift changes what a 40-minute appointment can achieve. A GP with a full pre-consultation summary can spend those 40 minutes on clinical reasoning, differential discussion, and treatment planning — not on asking “did you bring your school reports?”
Documentation after the consultation should include the clinical summary pack attached to the patient’s record, your clinical note, and the outcome (diagnostic impression, treatment plan, referral if applicable). The summary pack is the evidence base. Your clinical note is your reasoning. Both need to be in the record.
Common workflow failures and how to avoid them
| Failure | Why it happens | How to avoid it |
|---|---|---|
| Patient arrives without completing intake | No reminders, or forms too cumbersome to complete | Automated digital reminders 72 hours and 24 hours before appointment. Mobile-first form design. |
| Observer report never received | Paper forms lose. Phone calls take too long. | Digital invitation sent directly to the observer, with automatic reminders. |
| Childhood evidence absent | Patient not asked specifically, or asked too late | Upload request in the intake form with specific examples of what to upload. |
| GP opens appointment with no pre-reading time | Summary not available or not surfaced clearly | Dashboard with readiness indicator checked by GP or receptionist the day before. |
| Clinical summary not in the patient record | No download/attachment step in the workflow | PDF export to Best Practice or Medical Director. Practice nurse handles attachment for practices where this is appropriate. |
Practice manager checklist
If you are a practice manager setting up this workflow, here is the setup checklist:
- Confirm your state’s training requirements and that your GP has completed approved training
- Choose your pre-appointment intake tool and configure the GP’s profile (name, credentials, practice branding)
- Create a test assessment and complete it yourself as a patient to understand the patient experience
- Add reception and admin staff as team members (non-clinical seats, no access to patient clinical data)
- Set up your booking instructions so patients know to expect an intake link at the time of booking
- Confirm the PDF export workflow for attaching summaries to Best Practice or Medical Director
- Brief the GP on how to read the clinical summary before consultations — 10 minutes of pre-reading time should be blocked in the schedule
If you want to see exactly what this workflow looks like in practice, book a demo. Velluto was built with a practising GP to handle every step described above — from booking to consultation-ready summary — without manual work from your team.
Frequently asked questions
What does a complete GP ADHD assessment workflow need to include?
A complete adult ADHD assessment workflow needs to reliably collect five evidence components before the consultation: the ASRS v1.1 self-report questionnaire, an independently completed observer report, childhood onset evidence, medical and psychiatric history screening, and a structured clinical summary ready for the GP before the appointment. The consultation itself is then the clinical interview, not the data collection step.
How do you get an observer report for a GP ADHD assessment?
The most reliable method is a digital invitation sent directly to the observer by the intake system, without the patient acting as relay. The patient nominates the observer’s name and email address during their intake. The observer receives their own secure link, completes the 18-item DSM-5 questionnaire independently on their own device, and the scored results appear in the GP’s pre-consultation summary. Manual methods — paper forms, phone calls, asking the observer to attend — are significantly less reliable and create administrative work.
How much time should be allowed for pre-reading the clinical summary before an ADHD consultation?
Ten minutes is a reasonable minimum. The clinical summary for an adult ADHD assessment includes ASRS scores with subscale breakdown, observer report scores, extracted childhood evidence, inconsistency flags, differential diagnosis flags, and a gaps report. A GP who reads this before walking into the consultation is working from structured evidence. A GP who opens the appointment without pre-reading is starting from scratch.
Clinical information disclaimer
This article contains general clinical information for healthcare professionals. It is not a substitute for individual clinical judgement, professional guidelines, or specific patient assessment. Always apply your own clinical reasoning when making treatment decisions.
Velluto is a clinical intake platform. It does not diagnose, recommend treatment, or make clinical decisions. All clinical decisions remain with the treating GP.